
The Dynamic Remodeling Method is a non-surgical approach to treating pectus deformities using Dynamic Chest Compression (DCC) brace and exercises.
Treating pectus excavatum and pectus carinatum with this conservative method has been proven to work for years.
The external compressive brace modifies the malformed bone structure while exercising increases intrathoracic pressure, forcing the cavity to flatten.
This process has numerous benefits over surgery, especially in mild and moderate deformity cases.
Pectus and Orthopedics
There is a direct connection between orthopedics and pectus deformities. The conservative treatment method of pectus deformities is based on the principles of Nicolas Andry.
He is regarded as the father of orthopedics. The Law of Bone Remodeling can explain the development of the Dynamic Remodeling method by Julius Wolff, which goes by the following:
“Therapeutic forces that are regularly applied on deformed bones and cartilage can create gradual reshaping in a beneficial and corrective direction. This mostly applies to the anterior chest wall, which is a very flexible region in the human body.”
Julius Wolff
It would be best if you take some time to learn the basic orthopedic concepts, to understand better how the Dynamic Remodeling method works in correcting pectus deformities.
According to Dr. Sydney Haje and Dr. Davi Haje, the essence of pectus deformities should be a part of the study of orthopedic problems.
History
Doctors treated pectus deformities in the 1950s and 1960s only surgically. Surgeons neglected conservative treatment options as totally ineffective.
However, in the 1970s, pectus surgeries were criticized because of various cases of complications such as wound infections, hematoma, collapsed lungs, atelectasis (complete or partial collapse of the entire lung or a part of the lung), ugly scars across the chest, decreased in lung capacity and even death.
Surgeons constantly conflict and find problems with surgical techniques, and surgery modifications are always ongoing. More than 40 surgical procedures fix pectus problems, which means that the ideal surgical method isn’t yet produced.
In 1969, Lange and Müller had good results in treating young children that suffered from pectus carinatum with belt bracing.
Later, in the United States in 1993, a female adolescent patient with pectus carinatum was treated successfully with a plaster cast followed by bracing with a belt.
Since 1979, Dr. Haje and colleagues have treated pectus excavatum and pectus carinatum with a compression brace called Dynamic Chest Compressor (DCC).
There are two types of DCC braces. In some rare cases where the patient has a mixed type of pectus deformity, the concurrent use of both braces will be necessary.
Custom-Made Brace
According to Orthopectus, the DCC brace is ineffective unless it is custom-made for every patient and used for many hours throughout the day in addition to performing special exercises.
A doctor must examine the patient to determine the chest wall flexibility and see how fast it can be corrected using the Dynamic Remodeling Method.
The older versions of the brace were made by measurements or plaster, casting the deformity under the doctor’s control. For the treatment to be effective, the patient is given special instructions on using the brace and what exercises should be done.
The correction process is fully documented with pictures at the Orthopectus Clinic to see before, during, and after treatment. The doctor’s guidelines are essential to prevent complications such as overcorrection.
Two Braces
There are two types of DCC braces, used on two different occasions:
- DCC 1 orthosis – Produced in 1977 to treat patients with pectus carinatum
- DCC 2 orthosis – Produced in 1988 for patients with pectus excavatum
Over the last 40 years, these two models have been constantly improved throughout the years, to make the correction process simpler for both doctors and patients.
Construction
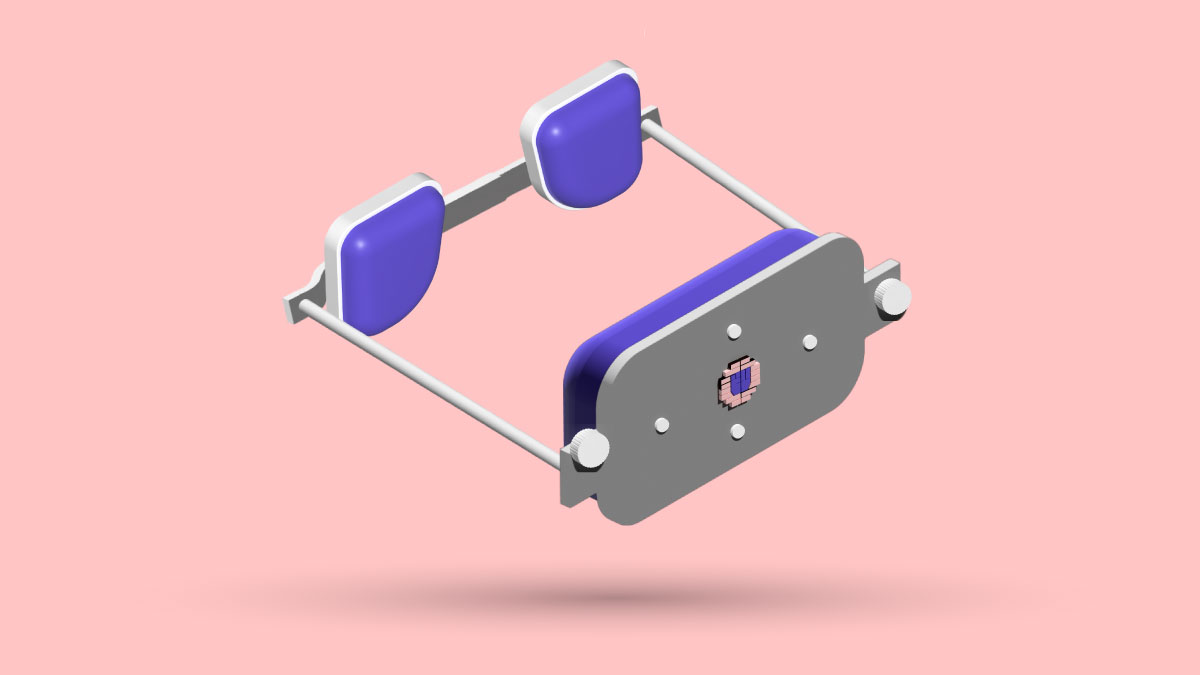
The compressive brace is constructed of two anterior cushions that compress and modify the flared ribs’ shape.
The two cushions are connected to a rear cushion with a threaded bar that allows you to easily adjust the compression force on the deformed bones and cartilage.
Dynamic Adjustable Chest Compressor
In late 2015, there was a significant update, and researchers introduced the Dynamic Adjustable Chest Compressor (DACC).
This increases the effectiveness of the Dynamic Remodeling method, and the treatment procedure for patients and doctors is more straightforward and effective.
Best Way to Treat Pectus
According to Dr. Sydney Haje and Dr. Davi Haje, the best scientifically proven method to reverse your pectus excavatum is the combination of compression of the costal edges (flared lowered ribs, typical in pectus excavatum) and the increase of intrathoracic pressure caused by exercising while wearing the brace.
Treatment
According to Orthopectus, it is best if the treatment for the pectus excavatum deformity starts as soon as the chest begins to sink in.
It is possible to have excellent results in just a few months with proper usage of the DACC 2 brace, combined with special exercises.
To maintain the treatment’s effectiveness, the patient must wear the brace. Continuation with the activities is advised until rapid growth is finished, usually at the end of puberty.
6 Factors for Success
The effectiveness of the treatment can differ a lot and relies on a few factors:
- The flexibility of the chest wall
- Type of pectus excavatum
- Patient’s age
- Whether the patient is disciplined and follows the treatment plan as written
- Correct guidelines of treatment given by the physician
- The doctor determines the psychological situation of the patient that will interrupt the treatment process
Flexibility
Even though it may be surprising, the anterior chest wall flexibility is more important than the deformity severity for the Dynamic Remodeling Method to succeed.
Do Chest Flexibility Test Manually


- Pectus Carinatum – Use the palm of your hand to compress the chest’s protrusion area. In contrast, the other hand supports the thoracic spine. The chest wall is flexible if the protrusion reduces.
- Pectus Excavatum –All you need to do is take a deep breath in a standing position while squeezing the abdominal muscles. Hold the air like you expect a punch to the stomach to increase intrathoracic pressure. At the same time, the tester should manually compress the flaring of both lower ribs. Don’t worry; this isn’t anything complicated.
Exercising
For the Dynamic Remodeling treatment to fix pectus excavatum or carinatum, the patient must do a few simple exercises to increase the chest’s intrathoracic pressure.
That will make balance the forces on the chest. The brace will put external pressure on the malformed, protruding bones of the chest wall.
At the same time, the exercises will cause internal pressure on the recessed area of the chest, promoting superior remodeling of the chest wall. Wearing the brace while doing the prescribed exercises is essential.
The patient should perform the exercises daily.
7 Main Exercises







Purpose
These exercises aren’t to build hypertrophy in the muscles but to create intrathoracic pressure and movement of the chest cavity. Orthopectus recommend these exercises.
Because of that, you shouldn’t lift a lot of weight. It would be best if you didn’t lift the weight but gradually increased the total number of repetitions.
Problem With Bodybuilding
According to Dr. Sydney Abrao Haje and Dr. Davi Haje, the sinking of the breastbone can become more rigid, and the bodily appearance will be worsened if there is excessive muscle mass in the pectorals.
This is a huge problem when improving your pectus excavatum appearance non-surgically. Exercises in the pushing pattern, such as the bench press, are often overused.
At the same time, the muscles in the back required for optimal posture are neglected, leading to muscular imbalance.
How to Do Exercises
The patient must perform the prescribed corrective exercises in the gym while wearing the brace.
Activities can be performed at home while wearing the brace when the patient doesn’t want to go to the gym. The peck-deck exercises should be executed three times a week while the patient wears the DCC brace.
Exercises to Do When You’re Not Wearing Brace
Some exercises like swimming are recommended if you suffer from pectus excavatum or carinatum at any age.
It will help you maintain chest wall flexibility and improve physical conditioning while helping enhance your posture. The most helpful types of strokes you should perform while swimming is:
- Backstroke
- Freestyle
- Crawl
Yoga and Pilates can also be beneficial.
Exercise Alone Isn’t Enough
According to Orthopectus, weight training, swimming, or any other exercise cannot correct the pectus excavatum or carinatum deformities alone. They can only increase muscle hypertrophy and improve poor pectus posture.
It is crucial to know that if you perform weight training without wearing the Dynamic Remodeling brace, the thoracic protrusion during the growth spurt will be worsened, and the bones will be hardened.
This will reduce the effectiveness of chest wall correction using chest compression because the bones will be harder to modify.
Medical Supervision
It is highly recommended the Dynamic remodeling method be performed under medical control for more than a year or until the patient isn’t in a growth spurt anymore.
The chest is corrected to the point where the patient is satisfied with the outcome. The physician should give the specific daily exercises and recommended schedule.
The Orthopectus physician and physiotherapist further explain the guides for exercises.
When Is this Method most Effective
According to Orthopectus, there are certain situations where the Dynamic Remodeling method is most effective.
- Pectus excavatum with flared ribs. Most people with sunken chest deformity also have flared ribs, which further worsens the chest wall appearance, making the sternum appear more sunken than it is. I had this type of pectus excavatum.
- Lateral type (asymmetric type) or Inferior type of pectus carinatum deformity
If you suffer from these two types of deformities, the chances of improvement are very high. You will feel more motivated to follow the treatment instructions for a long time because of a higher success rate.
Even if you don’t have these two types of deformities, you will see fantastic improvement if you are disciplined with the treatment procedure.
Problem With Surgery
According to Dr. Sydney Haje and Dr. Davi Haje, most surgeons consider surgery the only practical option to treat pectus excavatum. The problem with surgery is the cosmetic results aren’t always satisfactory.
Sydney Haje & Davi haje Opinion
If the patient is still growing, Dr. Sydney Haje and Dr. Davi Haje recommend starting with the non-surgical treatment of pectus excavatum correction with the Dynamic Remodeling method (braces and physical exercises).
This method is low risk, and the patient can change their mind during the treatment.
When to Undergo Surgery
According to Dr. Davi Haje at Orthopectus, doctors should only suggest surgery to patients who:
- Patients who tried the Dynamic Remodeling method previously without a successful outcome.
- Those with severe deformities that hinder the functioning of the heart and lungs.
- Patients with psychological problems result from body dissatisfaction, such as constant depression, anxiety, social anxiety, chronic stress, and low self-confidence.
how to Start DR Method
The researchers concluded that treating a localized and broad pectus excavatum with the Dynamic Remodeling method was successful in motivated patients.
There was no deformity recurrence after the patients finished the initial treatment during the study period and continued with the therapy until skeletal maturity.
This treatment is low-risk and relatively pain-free, allowing patients to quit if they aren’t interested in keeping up with the brace application and exercising regularly.
According to the researchers in this study, flexibility is described as a critical predictive factor in treating pectus excavatum with the Dynamic Remodeling method.
The subsequent studies showed that almost 50% of the patients had satisfactory results, especially those with mild and moderate types of deformity.
One of the studies is about a broad type of pectus excavatum, and the other is about localized pectus excavatum.
Broad-Type Pectus Study
Chest Flexibility Measurement
To measure the chest’s flexibility, an examiner must make a manual compression maneuver of the lower protruding rib cage in the front-to-back direction.
At the same time, the patient must perform the Valsalva maneuver (breathing out strongly through your mouth while keeping your nose closed) while squeezing the core muscles against arm resistance.
Younger patients are instructed to blow a balloon. This test can result in the patient’s deformities being listed as:
- Flexible – When there was a complete reversal of the patient’s chest hole.
- Moderately flexible – When there was a partial modification in the depression
- Stiff or inflexible – When the depression didn’t change or barely altered
Severity
Doctors list the severity of broad-type pectus excavatum as follows:
- Mild
- Moderate
- Severe
how Long Do Patients Wear Brace
Patients were required to wear the brace for 23 or no less than 18 hours at a minimum during the broad pectus excavatum study.
Patients were allowed to remove the brace while showering, swimming, or participating in contact sports. They were responsible for keeping the chest compression comfortable, not overcompressed or under-compressed.
They needed to manually adjust the brace to provide more compression when the lower rib flaring was minimized. Patients should do special exercises during the treatment to strengthen the chest muscles.
When they were finished with the Dynamic Remodeling treatment after 24 months, removing the orthosis was gradual because the patients depended on it for so long.
When patients did not wear the brace for the required amount of time in a day (at least 18 hours) or when they didn’t perform the required exercises while wearing the brace, doctors removed the patients from the study.
Three Outcomes
There were three classifications of the success of the Dynamic Remodeling method in the study:
- Poor – When the deformity doesn’t correct or even becomes worse.
- Average – When there was under-correction.
- Good – When there was a significant improvement.
Dr. Sydney Haje and Dr. Davi Haje were responsible for the examination and treatment outcomes of the study.
Patient Satisfaction
If the patient was a child, the parents were asked whether the non-surgical treatment was satisfactory. If the patient was an adolescent, they were asked about their satisfaction as “satisfied” or “not satisfied.”
If the patient was “satisfied” with the outcome, the result was defined as “good.” Also, before and after pictures were taken from the same positions and lighting.
Researchers did this to compare the visual differences of the anterior chest wall.
Simplifications of Results
AGE & SEX
At the start of the study, the 84 treated patients had:
- The median age of 13.3 years
- 66 were male, 18 were female
SEVERITY OF DEFORMITY BEFORE TREATMENT
- 11 patients (13%) – mild
- 55 patients (66%) – moderate
- 18 patients (21%) – severe
Initial Deformity Flexibility
- 50 patients (59%) – Very flexible or relatively flexible
- 34 patients (41%) – Rigid or not very flexible
RESULTS AFTER THE STUDY:
- 40 patients (48%) – good results
- 36 patients (43%) – average results
- Eight patients (9%) – poor results
TREATMENT SATISFACTION
- 40 patients (48%) were satisfied with the outcome
- 17 patients (20%) of the patients with average results
- 0 patients (0%) of the patients with poor results
Out of 84 treated patients, 57 were completely satisfied with the results.
GOOD QUALITY OF RESULTS
- Eight patients (72%) with mild deformity
- 26 patients (47%) with moderate deformity
- Six patients (33%) with severe deformity
The study concluded that the Dynamic Remodeling method for correcting pectus excavatum non-surgically was best for mild deformity cases.
GOOD RESULTS REGARDING FLEXIBILITY
- In 24 patients (48%) with a flexible or moderately flexible deformity
- In 16 patients (47%) with rigid or less flexible deformities
When these criteria were analyzed by Dr. Sydney Haje and Dr. Davi Haje, in isolation or with the discipline of brace use and exercise performance, they saw no meaningful difference between the results.
BRACE USE CONSISTENCY
- 58 patients (69%) were using the brace as prescribed
- 26 patients (31%) weren’t using it regularly
EXERCISING CONSISTENCY
- 45 patients (54%) performed the corrective exercises regularly
- 39 patients (46%) – weren’t performing them regularly
70% of patients who used the brace regularly and performed the corrective exercises regularly achieved good results.
On the other hand, only 29% of the patients achieved good results when they weren’t using the brace regularly, regardless of whether they exercised regularly or not.
This means that wearing the brace is extremely important if you want to correct the pectus excavatum deformity. You can’t achieve good results if you don’t wear the brace daily.
COMPLICATIONS
During the study, there weren’t any significant complications. Only 4% of all patients had slight skin irritation or transient hyperpigmentation at the places where the brace was compressing the body.
12% of the patients reported discomfort on the compression spot, which the patients solved quickly by reducing the pressure.
These side effects didn’t stop the everyday use of the brace during the 24 months. Contrary, some patients who use the vacuum bell treatment method cannot continue the treatment if their skin rashes don’t disappear for a few days.
HYPERCORRECTION
In two patients, hypercorrection (when pectus excavatum turns into pectus carinatum) was present. Reducing the DCC II brace usage time (the pectus excavatum compression brace variant) was necessary to fix this.
The patient was given a second brace, DCC I (for pectus carinatum correction). This complication was later corrected with this method.
Overcorrection proves that the Dynamic Remodeling method can effectively treat the pectus excavatum deformity without expensive surgery.
Localized PE Study

This study wanted to discover the effects of using a brace and performing specific exercises to correct localized pectus excavatum non-surgically.
Localized pectus excavatum is a deformity where the recessed area is confined only to the midline area along the nipple line.
There are no other studies on pectus excavatum treatment with braces and specific exercises while wearing the brace other than the studies of Dr. Haje.
Patient Ages
The age of the patients evaluated in the localized pectus excavatum study was between 2 and 19. The mean age at the start of treatment was 12.9 years.
To complete the treatment, the patients or their parents must be motivated to use this conservative method to fix the deformity. Most patients had moderate and severe deformities, while mild cases were also present.
The patients had to wear a brace and perform specific exercises to strengthen the torso muscles.
Like the patients in the broad type of pectus excavatum study, the patients in the localized PE study mentioned above were required to wear a brace for 23 hours in the day, or at least 18 hours.
List of Exercises
The patients were required to perform exercises five times a week, keeping maximal inspiration during the concentric contraction. The activities for the older patients and adolescents were:
- Push-ups
- Sit-ups
- Crucifix hold and crunch
- Trunk extension in a pronated position
- Blowing a balloon for ten minutes
Treatment Results Simplified
SEVERITY
- 34 patients (30%) had a mild case of deformity
- 67 patients (58%) had a moderate deformity
- 14 patients (12%) had severe deformity
FLEXIBILITY
- In 64 patients (56%), the deformity was very or moderately flexible
- Rigid or poorly flexible in 51 patients (56%)
RESULTS
- Good in 66 patients (58%)
- Average in 36 (31%)
- Poor in 13 (11%)
SATISFACTION
- Patients were satisfied with the outcome in all good results.
- Nine patients (25%) with average effects were satisfied.
- None with poor results were pleased.
REGARDING SEVERITY
- Good results were reported in 20 (57%) of patients with mild deformity,
- 41 or (61%) of patients with moderate deformity
- Five or (36%) of patients with severe deformity.
IN TERMS OF FLEXIBILITY
Good in 35 patients (55%) with flexible or moderately flexible deformities and 31 patients (61%) of patients with rigid or poorly flexible deformities.
CONSISTENCY OF BRACE WEAR
- Only 72 patients (63%) used the brace regularly.
- 43 patients (37%) irregularly
EXERCISE FREQUENCY
- Only 57 (49%) of patients were doing the specific exercises regularly
- 58 patients (51%) were doing them irregularly
FLEXIBILITY AND SUCCESS RATE
When the pectus excavatum deformity was flexible and regular bracing and exercising were done, excellent treatment results were evident, with 83% of patients having good results.
However, if the patient wore the brace irregularly but did the specific exercises, only 38% had good results.
On the other hand, when the patient wore the brace regularly and did the exercises consistently, good results were evident in 62% of all patients.
Complications
The complications were similar to the Dynamic Remodeling study on localized or broad pectus excavatum types.
Vacuum Bell and Brace

Scientific evidence proves combining vacuum bell therapy with braces provides better corrective improvement.
According to Ortopedia e Traumatologia: Princípios e Práticas book, where a chapter is written by Dr. Sydney Haje and Dr. Davi Haje, it is considered that the vacuum bell treatment can be utilized in cases of pectus excavatum as an additional treatment to the Dynamic Remodeling method, particularly in patients in which the chest depression does not have wholly satisfactory or slow initial results with primary therapy.
PUX-PEX and DR Method
There are seven models of vacuum bells that patients can try at Orthopectus, and physicians will tell you which size fits you most before purchasing.
Orthopectus recommend combining vacuum bell therapy with bracing and exercises for faster and better results.
Can Complications Occur?
If the treatment approach is wrong, there is a slight chance of possible complications. This is why being guided by a doctor throughout the process can be very important.
Dr. Sydney Haje and Davi Haje from the Orthopectus clinic stated that the most common complication is overcorrection.
They said it could happen in both pectus excavatum and pectus carinatum patients. Luckily, this can be corrected and inverted with proper treatment.
Overcorrection
Overcorrection usually happens in very motivated patients with flexible deformities who are willing to do whatever it takes to correct the pectus excavatum without surgery.
WHY YOU SHOULDN’T WORRY
You shouldn’t worry too much about overcorrection because it is far less frequent in cases of pectus excavatum.
For example, in the previously mentioned study, out of 17 patients with overcorrected pectus deformities who did Dynamic Remodeling therapy, only two had pectus excavatum.
OVERCORRECTION IN 30 PATIENTS
A study was published in 2006 by Dr. Sydney Abrao Haje and Dr. Davi Haje to demonstrate that overcorrection can happen during non-surgical treatment of pectus excavatum and carinatum.
The study reported that out of 3028 children and adolescents diagnosed with pectus deformities, Dynamic Chest Compressor (DCC) brace had been prescribed to 1824 patients.
After just a few months of therapy, overcorrection was reported in 30 patients out of 1824. However, the overcorrection was reversed successfully after that. Amazingly, the treatment was successful in all 1824 patients.
According to the study’s authors, pectus excavatum overcorrection with a non-surgical therapy is new, mainly because researchers initially thought patients couldn’t correct this deformity without surgery.
Skin Irritation
The best way to minimize skin irritation problems caused by the compression brace is to wear tight cotton clothing underneath the brace, so the brace doesn’t make direct skin contact.
Also, you can get cotton threaded covers with elastic edges around the compression pads. If you use these, you should wash them at least every other day to keep hygiene and stop bacteria buildup from the sweat that will probably accumulate because of the daily exercise with the brace on.
The skin irritation is more severe in the vacuum bell treatment because the thin silicone is always in direct contact with your skin. On the contrary, it is easier to care for your skin with the DTC brace.
How Tight to Put Compression Brace
When you feel chest pain or discomfort, you should loosen the brace compression, but make sure you don’t remove it.
When the discomfort disappears, you should tighten the screws to the point your physician previously estimated.
You should always feel comfortable with tightness and compression; You shouldn’t tolerate any pain or discomfort because it will demotivate you to wear the brace throughout the day.
There are infrequent circumstances where painkillers are given to the client.
Medications
Topical medications (medication spread to a particular location on the chest) are rarely required. In the cases where this is needed, you should follow the steps:
- The patient should apply the medication on the spot of skin irritation,
- Wait about two hours,
- Remove the oily cream or lotion with alcohol,
- Put the compression brace on again.
Can Deformity Reoccur?
The Dynamic Remodeling method is very similar to orthodontics in dentistry, which specializes in treating patients with improper positioning of the teeth. Dental braces are never used for just two months.
Similarly, patients with pectus excavatum need to wear the brace for a prolonged period, so the external brace compression and the intrathoracic pressure can modify the deformed bone structure of the chest.
Four factors come into play in whether the deformity may reoccur:
- Patient’s age
- Deformity flexibility
- Type of pectus excavatum or carinatum
- How disciplined is the patient in wearing the brace and performing the special exercises
Wear Brace While Sleeping
The patient must wear the brace as much as possible. It is recommended to wear it while sleeping during the first month. This is done so the patient gets used to the brace’s external pressure on the deformed chest structure.
If the patient can wear the brace for at least a month without quitting, the chances of success are increased, and cases of reoccurrence after the treatment is finished are significantly reduced.
The patient shouldn’t just stop wearing the brace when the deformity is corrected, and the treatment is completed after more than a year.
They should gradually discontinue the brace use, and medical supervision at Orthopectus is usually recommended, so the deformity doesn’t reoccur. This can lead to permanent pectus excavatum or carinatum correction.
Ideal Period for Dynamic Remodeling
According to Orthopectus, the best time to start the Dynamic Remodeling method is as soon as the chest indentation appears, usually during childhood and puberty.
Increase Effectiveness in Children
Young patients with pectus excavatum are recommended to:
- Blow balloons
- Participate in swimming and perform backstroke, crawl, and breaststroke strokes to improve chest wall flexibility.
How Children Can Achieve Better Success
To prepare children with pectus excavatum and flared ribs for the Dynamic Remodeling method, instruct them to blow bubbles with a straw in a glass filled with water.
This is a first and easy step to teach kids the blow exercise. The following exercise will be balloon blowing, with simultaneous manual compression on the deformed protruding areas of the ribs, in addition to abs strengthening exercises and swimming.
A kid with pectus excavatum needs to reach adolescence with less protruding ribcage, a more miniature concaved chest, and a more flexible chest that doctors will easily modify with the DCC 2 orthosis.
Finger Pressure
As stated by Orhotpectus, minimal finger pressure on the deformed ribs is recommended on babies with visible rib flaring and pectus excavatum.
The pressure should be applied using your thumbs, in a short time, with temporary interruption pauses of 5-10 seconds.
Because the chest wall of babies is very flexible, even thumb pressure will be enough to depress the rib flaring. If your baby is comfortable with this, you can repeat it 10, 20, 30, or more times.
The best time to do this is following a bath when the baby is thoroughly dried.
Complimenting Surgery With DR Method
The Dynamic Remodeling method will benefit the pectus excavatum deformity that reoccurs after surgery.
Orthopectus specialists have already done that, with a 100% success rate in two patients with pectus carinatum and partial success in four patients with pectus excavatum.
This will help many patients who aren’t willing to undergo painful surgery for the second time.
DR Method for Adults
Yes, the Dynamic Remodeling method can be effective in adult patients. However, correcting an older patient’s deformity is more complex than an adolescent patient, but it is still possible.
An essential factor is an anterior chest wall flexibility. Because of that, a chest wall flexibility test needs to be done.
Patients can use the Dynamic Remodeling method effectively if the test yields positive results and the deformity is flexible. Usually, adults don’t have a very flexible deformity.
However, consistent application of a brace and performing exercises can help increase chest wall flexibility.
Increase in Interest
Nowadays, more and more adults are interested in DCC braces. Orthopectus started suggesting this type of conservative therapy for them, with great success, especially in highly motivated patients to follow the treatment plan.
Orthopectus began treating adult patients with pectus deformities in the late 1990s. More sacrifice and motivation are often needed for this non-surgical therapy to work effectively in adults.
However, most adults usually have more willpower and discipline than adolescents.
Because of that, they probably wear the brace as prescribed and do the corrective exercises daily. Also, when the treatment is finally finished and the chest is corrected without surgery, they feel great accomplishment and are proud that the hard work paid off.
49-Year-Old Patient Success
At this time of writing, the oldest treated patient at Orthopectus is 49 years old, with a complete deformity correction. After the successful treatment with the DR method, the patient said he felt like he was born again.
However, he admitted that he went through a somewhat aching transformation but decided to continue the therapy until he overcame the fear and insecurity he had faced all his life.
Success Is Lower in Adults
There are a few reasons why the success rate in treating pectus excavatum with the Dynamic Remodeling method is lower:
- Inflexible anterior chest wall
- Reduced bone reshaping capability
- Social and professional obligations that lead to shortened use of a brace
- Unnatural to adapt to the brace, especially while sleeping
Can Weight Training Without Brace Fix It?
According to Orthopectus, weight lifting alone without braces can make the pectus deformity worse and stiffer, which will be harder to improve.
They highly recommend that adolescents and grown-ups perform exercises only while wearing a pectus brace. Like many people think, gaining muscle mass can only make the deformity less noticeable and doesn’t repair the bone and cartilage.
Orthopectus doesn’t recommend bodybuilding or weightlifting for patients who don’t use the DCC braces. The only exception is when they combine wearing the DCC brace while weightlifting.
Performing gym exercises without collateral use of DCC braces can make the pectus carinatum worse and do absolutely nothing to fix the pectus excavatum other than camouflaging it by adding muscle mass in the muscles around the indentation.
The goal of the Dynamic Remodeling method is not to increase the size of the muscles but to spread proportional forces to the deformed location. It is essential to wear a brace while exercising.
Orthopectus Recommends Swimming
Swimming is the only type of exercise that Orthopectus doctors recommend without a brace or prior examination at their clinic.
Even though swimming will not fix the deformity by itself, it will not stiffen or deteriorate the bone structure of the deformation.
A clear example of this is the Olympic swimmer Cody Miller. Looking at his chest, you can see that the muscles only make it less noticeable. The indentation is still apparent.
Weakness in the thoracoabdominal muscles can worsen the pectus deformities if the patient is still growing. On the other hand, the thoracic wall musculature is very well developed in swimmers.
Doctors at Orthopetus believe that strengthening these weak muscles by swimming while the thoracic wall is still growing can prevent aggravation of the deformation.
Does Brace Affect Breathing?
When the DCC brace is constructed correctly, it shouldn’t hinder natural breathing.
The researchers at Orthopectus reported cases where there was an improvement of respiratory problems such as asthma in patients when they improved their pectus excavatum condition using the Dynamic Remodeling method.
At first, you will feel uncomfortable when you wear the brace. You may feel a slight restriction in natural breathing; however, this will go away shortly because you will get used to the compression.
When to Take Brace Off?
You should remove the brace when you’re showering, swimming, or participating in a contact sport like basketball, football, soccer, etc.
However, it would be best if you remembered to put the brace on immediately after finishing the contact activity.
It is vital to make this a habit, as you will increase the brace wear time throughout the day, leading to faster correction of pectus excavatum.
Remember that it is your responsibility to wear the brace as much as possible because doctors only give instructions on using it. Discipline is critical for successful treatment.
DR Method Without Consulting Orthopectus?
According to Orthopectus, it is possible; however, it won’t be so simple because the patient’s problems may require medical supervision to be effective.
Many physicians do not understand their method correctly, especially for treating pectus excavatum. They have even seen cases where patients received improper braces, worsening the deformity.
Biggest Mistakes
- Being given a brace not constructed according to the patient’s body structure
- Braces built without prior photo documentation
- No programming and regulations whatsoever
- Not being given exercises to perform while wearing the brace
The most important thing for a brace to be effective is to be in the correct shape and positioned correctly on the patient’s deformed bone structure.
The use of adjustable screws so that the patient can regulate the external pressure is essential. Velcro straps or side fasteners don’t work as adjustable compression. It’s simply not enough.
Conclusion
The Dynamic Remodeling method is a scientifically proven non-surgical way to treat pectus deformities. The side effects are minimal, and there is a high success rate, especially in patients with flexible mild or moderate deformities.
You can even combine the DR method with vacuum bell therapy to speed up the process of non-surgical correction.
The life quality of the patients will improve because living with a Nuss bar underneath the sternum for three years can be irritating.
If you have any concerns, please leave a comment below. Feel free to contact me or contact Orhtophectus directly. Thank you for reading!
11 Sources
- Nicolas Andry. In: Wikipedia [Internet]. 2022 [cited 2022 Dec 1]. Available from:
https://en.wikipedia.org/w/index.php?title=Nicolas_Andry&oldid=1082164621 - Wolff’s Law: Physical Therapy, Workouts, and More [Internet]. [cited 2022 Dec 1].
Available from: https://www.healthline.com/health/wolffs-law#takeaway - Haje SA, de Podestá Haje D. ORTHOPEDIC APPROACH TO PECTUS DEFORMITIES: 32
YEARS OF STUDIES. Rev Bras Ortop. 2015 Nov 16;44(3):191–8. - Haje SA, Haje DP. Overcorrection during treatment of pectus deformities with DCC orthoses: experience in 17 cases. Int Orthop. 2006 Aug;30(4):262–7.
- Pectus Brace : Remodeling Method | Clinical Center Orthopectus [Internet]. Orthopectus. [cited 2022 Dec 1]. Available from: https://orthopectus.com.br/eng/the-dynamicremodeling-method-dr-method-clinical-center-orthopectus/
- Pectus Excavatum Treatment | Clinical Center Orthopectus [Internet]. Orthopectus.
[cited 2022 Dec 1]. Available from: https://orthopectus.com.br/eng/pectus-excavatumclinical-center-orthopectus/ - Frequently Askd Questions | Clinical Center Orthopectus [Internet]. Orthopectus.
[cited 2022 Dec 1]. Available from: https://orthopectus.com.br/eng/frequently-askdquestions-clinical-center-orthopectus/ - HAJE DDP, HAJE SA, VOLPON JB, SILVA ACOD, LIMA LFB, HUANG W. LOCALIZED PECTUS EXCAVATUM TREATED WITH BRACE AND EXERCISE: LONG TERM RESULTS OF A BRAZILIAN TECHNIQUE. Acta Ortop Bras. 2021;29(3):143–8.
- Haje D de P, Haje SA, Volpon JB, da Silva ACO, Lima LFB, Huang W. BROAD PECTUS EXCAVATUM TREATMENT: LONG TERM RESULTS OF A BRAZILIAN TECHNIQUE. Acta
Ortop Bras. 2021;29(4):197–202. - Hebert S, Filho TEPB, Xavier R, Junior AGP. Ortopedia e Traumatologia: Princípios e
Práticas. 5a edição. Artmed; 2016. - Tratamento de Pectus em Adultos [Internet]. Orthopectus. [cited 2022 Dec 1]. Available from: https://orthopectus.com.br/tratamento-de-pectus-em-adultos/












